
Pain is a universal experience. It’s a feeling of physical discomfort that results from illness or injury and is often the first signal that there is something wrong. But, pain manifests in many different ways. There are varying pain levels depending on the extent of an injury sustained or the severity of a condition. Pain levels can be felt in a wide range of feelings, from a mild sensation that’s more annoying than painful to paralyzing pain that prevents mobility.
Pain is also the body’s way of saying that you might need to stop doing certain physical activities that aggravate the condition. For example, the pain emanating from a sudden ankle sprain becomes more pronounced every time the ankle is moved. The more severe the sprain, the more painful the signal. Or, pain can also signal the body to start doing something to prevent more damage from happening. An example would be if a body part comes into contact with an open flame. The slightest sensation of pain tells the brain to do something to protect the body. In most cases, the reaction would be instantaneous.
Importantly, pain lets you know something is wrong. The many pain sensations all share the same thing: the body is requiring attention. Sensations include feelings of soreness in certain body parts (tired legs) or diffused throughout the whole body (fatigue). There are also short bursts of pain ranging from stabbing (stomach cramps) to throbbing (headache) sensations. Also, pain results from extreme experiences of hot and cold, such as burns or frostbite.
Acute and Chronic Pain

In general, pain can be described as acute or chronic. When pain is experienced for a short period, between a few minutes to around three months, it is usually classified as acute pain.
Pain emanating from soft-tissue injuries or a passing sickness is often temporary and thus termed acute. It is often described as sharp or severe, and it can last between a few seconds or linger for hours.
On the other hand, pain that persists for more than three months, whether constant or intermittent, is called chronic. This type of pain is usually the result of a lingering illness (cancer) or a similar chronic condition like arthritis, scoliosis, or fibromyalgia. Note that acute pain, if not addressed properly and on time, can graduate into chronic pain.
Other Types of Pain
Apart from classifying pain into acute and chronic, pain can also be classified based on where the pain comes from. Pain can be termed neuropathic, nociceptive, or radicular pain. These pain types can either be acute or chronic.
Neuropathic pain
Neuropathic pain is pain generated by damage to the nervous system. It is characterized by a sensation often described as feeling like being jabbed by a million tiny pins and needles all over the affected area simultaneously. Neuropathic pain also affects touch sensitivity, making it more difficult to determine hot or cold feelings.
Nociceptive pain
Nociceptive pain is the pain felt when body tissue is injured often caused by external injuries. Nociceptive pain is felt in the joints, tendons, skin, muscles, and bones. This type of pain can be either chronic and acute. Good examples of nociceptive pain would be head injury, muscle sprain, and bone fractures.
Radicular pain
Radicular pain is a very particular kind of pain that is caused by an inflamed or compressed spinal nerve. The pain is described as radiating, originating from the back or hips and into the legs via the spine and spinal nerve root. Back pain or pain that radiates from the back into the leg is called radiculopathy. This condition is usually identified as sciatica, as it is often the sciatic nerve that is the culprit.
The Problem With Describing Pain

Diagnosing the cause of pain often requires the medical practitioner to ask patients to describe the pain. Usual questions include where the pain is coming from, is it constant or intermittent, and whether the pain prevents the sufferer from performing regular activities. Most importantly, doctors and medical staff need to know how much pain is being felt. Only then can they suggest interventional pain treatment solutions.
This is where the issue lies. According to the National Institute of Health, pain is a subjective feeling. Asking a patient to describe their pain, as well as taking in the evaluation of an observer can be influenced by many factors. This includes socio-economic status, beliefs, and psychological status. For example, the same injury can produce different results depending on a number of factors. A person distracted by a task or in a hurry to get somewhere might be more inclined to shrug off an injury compared to others.
Pain’s subjectivity prevents an accurate assessment of the patient’s condition. What can be very painful for you can be mildly painful for others, or vice versa. In addition, as pain is a personal experience, it can be difficult to communicate accurately. At the same time, medical personnel recording the information may find it similarly difficult to translate to an objective report. Measuring the degree of pain is critical for both medical staff and the patient in pinpointing likely causes and in coming up with solutions.
How Do You Measure Pain?
While medical science developed a number of methods to document pain felt by patients, there remains a lot to understand about pain. Its subjectivity actually inhibits scientists from developing tools to accurately quantify pain. But, over the centuries, attempts have been made on the subject.
Schmerzpunkte
One of the earliest documented attempts to measure pain came in 19th century Germany. The discipline called “psychophysics'' studied the relationship between stimuli and sensation. Scientist Maximilian von Frey developed a method to measure what he called Schmerzpunkte (pain points). He would select horse hairs of varying stiffness and attach them to individual sticks. He would then press the hair from each stick against a subject’s skin. Using this method, Von Frey documented the amount of pressure that can cause a person to feel pain from a particular hair. Von Frey and his psychophysics colleagues also tested other methods to test skin sensitivity. This includes employing hot or cold rods of varying temperatures.
Dolorimeter
Fast forward a few hundred years, when a group of researchers tried to pick up where psychophysics left off. James Hardy, Helen Goodell, and Harold Wolff, all from Cornell University, developed a pain measuring device in the 1940s that they called the dolorimeter. They invented the device to help evaluate the effectiveness of analgesics. Dolorimeters apply steady heat, pressure, or electricity to an area of the body to determine the pain thresholds and pain tolerance of patients. Their studies showed that on average, subjects reported pain sensations at a skin temperature starting 113 °F (45 °C). Also, they found that after a certain threshold of 152 °F (67 °C), pain sensations did not intensify even if the heat was increased.
Using the results of the study, the researchers developed the "Hardy-Wolff-Goodell" scale, with 10 levels called dols. However, other research teams weren’t able to duplicate their study, so the idea of dolorimeters was abandoned. But, they did manage to point scientists in the right direction.
Modern Pain Scales
With the advances of modern sciences developing alongside a growing awareness of medical ethics, the methods for measuring pain became less invasive and avoided inflicting any sort of bodily harm to subjects. Instead, patients are simply asked to describe their pain, and the date will then be recorded and set against established standards. While they remained subjective, this gives medical practitioners more information on the degree of pain being felt.
There are three basic categories of pain scales. These are categorized based on the input data required to complete the assessment.
- Numerical Rating Scales (NRS) use numbers to rate pain. Patients are usually asked to select a number from a given scale that best describes the degree of pain felt.
- Visual Analog Scales (VAS) utilize a scale where patients are asked to mark where they think their pain levels are closest.
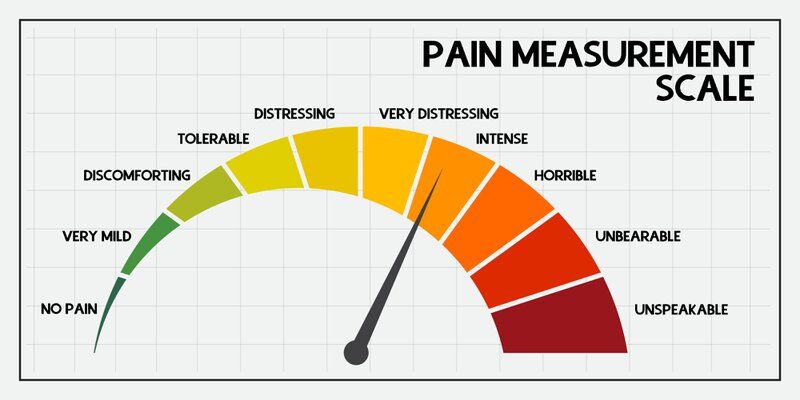
- Categorical Scales use words to describe the pain levels. They may use numbers, colors, or relative locations to communicate pain.
While numerical rating scales are quantitative and visual analog and categorical scales are qualitative, one type does not automatically mean it’s better than the others. Pain measurement often requires both quantitative and qualitative data for a more accurate diagnosis.
10 Pain Scales and How They Measure Pain Levels
Numerical Rating Pain Scale
The Numerical Rating Pain Scale is a simple pain scale that grades pain levels from 0 (No pain), 1,2, and 3 (Mild), 4,5, and 6 (Moderate), 7,8, and 9 (Severe) to 10 (Worst Pain Possible). This simple tool assumes a grasp of basic number skills and is recommended for patients over the age of nine.
Patients will need to rate three kinds of pain: Current, Best, and Worst Pain experienced within the past 24 hours. Medical personnel will get the average of the three ratings and use the answer to represent the patient’s current pain level.
Wong-Baker Faces Scale
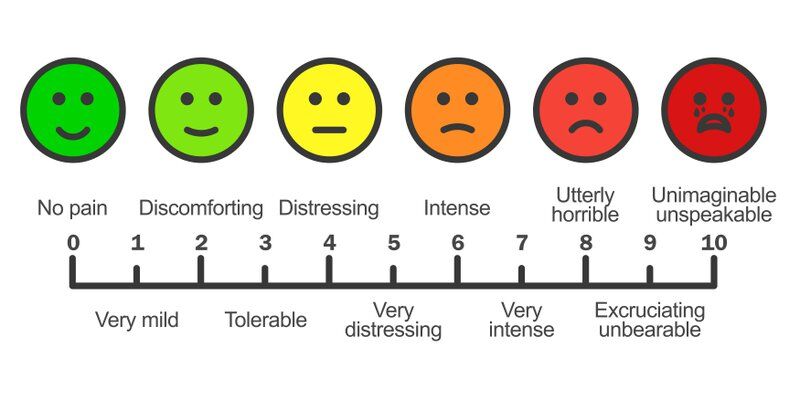
The Wong-Baker Faces Scale uses faces that run the course of emotions from Smiling (0, or no pain) to Crying (10, worst pain). It was developed by Drs. Donna Wong and Connie Baker. This tool further simplified the numerical rating of pain by assigning a graphic to each number on the pain scale.
The Wong-Baker Faces Scale was developed to assist children in providing the level of pain being felt. This has been tested to work with patients 3 years old and above. It also works well with illiterate patients or those who have verbal abilities. It also provides a culturally-sensitive depiction of the human face.
FLACC Scale
The FLACC (Face, Legs, Arms, Crying, Consolability) scale is a behavioral pain assessment tool used to help determine pain levels in nonverbal or preverbal patients who lack communication skills to report their own pain levels. Doctors and other qualified medical staff can assess a patients’ pain levels by observing the 5 FLACC categories. They use a pre-made form to fill out scores (0, 1, or 2) that best describes the patient’s condition. The FLACC pain scale is a valuable tool for assessing infants and children between two months and 18 years of age. They are also very useful for children with existing cognitive impairments or developmental delays caused by disease or earlier conditions.
COMFORT Scale

The COMFORT scale is a measurement tool used by healthcare providers to measure pain levels in patients that are unable to perform a self-check. They are suitable for infants and children, incapacitated or cognitively impaired adults, and sedated or ICU-confined patients.
The COMFORT Scale provides a pain rating between 1 (low) to 5 (high) on a total of nine categories:
- Alertness
- Calmness / Agitation
- Respiratory Response
- Blood pressure
- Heart rate
- Muscle tone
- Crying
- Physical movement
- Facial tension
Note that some versions of the COMFORT scale may have a different number of categories. In some cases, some categories were grouped together.
Visual Analogue Scale
The Visual Analogue Scale (VAS) is a tool used to measure pain a patient feels that removes the perceived “jumps” from none, mild, moderate, and severe. The VAS was developed to conform to the patient’s perspective that the pain they feel is continuous and not something that shifts abruptly.
The simplest variation of the VAS is a single 100 mm line between No Pain to Very Extreme Pain. The patient is then asked to mark a point in the line corresponding to the level of pain they’re experiencing. The VAS score is determined by measuring in millimeters starting from the left end to the mark. Other variants of the VAS, including a vertical line and lines with descriptors, have been developed.
McGill Pain Questionnaire
The McGill Pain Questionnaire is a list of 78 adjectives that help patients describe the pain they’re feeling. Designed for literate patients, they can be useful in developing a rehabilitation plan, as they pinpoint the range of pain being felt. Patients need to mark the words that closely resemble their pain levels. Medical staff will then assign the patient with a score (not exceeding 78) based on how many words were marked.
Defense and Veterans Pain Rating Scale (DVPRS)

The DVPRS is a relatively new scale developed by the Department of Defense for use in military hospitals to better assess pain in patients. It combines the Wong-Baker pain scale of 0-10 with an assessment tool that measures the pain’s impact on patients’ daily function. In addition, the DVPRS contains additional questions that help determine the effects of pain on a patient’s daily functions like activity, sleep, mood, and stress.
Pain Assessment in People With Dementia (PAINAD)
Many older adults lose the ability to communicate clearly, especially those suffering from dementia. Comprehensive pain specialists will find it difficult to determine their levels of pain using conventional scales. PAINAD was designed to assess pain in Dementia patients based on five specific indicators: breathing, vocalization, facial expression, body language, and consolability. Similar to FLACC, each category contains three choices ranging from 0 to 2. A trained health professional can use the PAINAD scale to assess patients within five minutes of observation.
Behavioral Pain Scale (BPS)

The Behavioral Pain Scale is a simplified version of the McGill Pain Questionnaire. It helps assess pain levels in sedated or mechanically ventilated critically ill patients. The scale works well for patients that cannot communicate at present due to their condition. BPS consists of three items (Facial Expression, Upper Limbs, and Compliance with Ventilation) with four distinct choices each. Health care providers only need to check the value that closely resembles the patient’s current behavior.
Mankoski Pain Scale
The Mankoski Pain Scale, developed by Andrea Mankoski in 1995, is a popular pain scale that provides well-defined states of pain. Designed for conscious patients that have moderate literacy skills, it can provide a narrower state of pain levels. Patients simply choose a number between 0 (Pain-free) to 10 (Unconscious) to describe their current state. Mankoski generously shared the pain scale with the public for free as long as attribution to the author is given. The Mankoski Pain Scale categories are:
- 0 – Pain-free
- 1 – Very minor annoyance – occasional minor twinges. No medication needed.
- 2 – Minor Annoyance – occasional strong twinges. No medication needed.
- 3 – Annoying enough to be distracting. Mild painkillers take care of it. (Aspirin, Ibuprofen.)
- 4 – Can be ignored if you are really involved in your work, but still distracting. Mild painkillers remove pain for 3-4 hours.
- 5 – Can't be ignored for more than 30 minutes. Mild painkillers ameliorate pain for 3-4 hours.
- 6 – Can't be ignored for any length of time, but you can still go to work and participate in social activities. Stronger painkillers (Codeine, narcotics) reduce pain for 3-4 hours.
- 7 – Makes it difficult to concentrate, interferes with sleep. You can still function with effort. Stronger painkillers are only partially effective.
- 8 – Physical activity severely limited. You can read and converse with effort. Nausea and dizziness set in as factors of pain.
- 9 – Unable to speak. Crying out or moaning uncontrollably – near delirium.
- 10 – Unconscious. Pain makes you pass out.
Describing Pain is Just the Beginning

There are many methods available to communicate pain levels being experienced to medical professionals such as comprehensive pain specialists. Once the pain is identified, it becomes easier for health care professionals to prescribe treatments.
Pain is often the signal that there’s something your body wants to tell you urgently. If you are experiencing pain that won’t go away, let Midsouth Pain Treatment Center take a look at your problem. We know that pain is a different experience for every person, so we’ll take time to get to know your conditions before we offer any solution.
Book an appointment or send us an email, we’ll help you find out the cause of your pain, and help you get back on your feet. Visit our site or come see us soon.
Articles from Midsouth Pain Treatment Center










